Ebola Outbreak in Congo Went Unnoticed for Weeks
The Ebola outbreak in Congo has exposed a troubling failure: by the time anyone formally raised the alarm, the virus had already been spreading silently for weeks. When the disease was finally identified in the Democratic Republic of Congo and Uganda in mid-May, the scale of the crisis was immediately apparent — hundreds of suspected cases and dozens of suspected deaths had already accumulated.
The World Health Organization moved quickly once the situation became clear, declaring the outbreak a public health emergency of international concern. But that declaration came only after the virus had been quietly circulating, leaving health officials racing to catch up with a crisis that was already well advanced.
A Surveillance System That Failed
Congo is not unprepared for Ebola. The country has battled some of the deadliest outbreaks in history and has invested in additional laboratories in recent years, building surveillance systems specifically designed to catch outbreaks early enough to contain them.
Yet this time, the system broke down. In Ituri Province, the epicenter of the outbreak, officials did not sound the alarm when patients first began showing symptoms. Critical samples appear not to have reached the capital, Kinshasa, for testing as quickly as they should have.
Dr. Marie-Roseline Belizaire, the epidemiologist leading the WHO’s response, said the alert came far too late. Normally, sharp increases in cases are flagged early by health officials or picked up in news reports. This time, weeks passed before authorities could confirm what they were dealing with.
Congo’s own scientific leadership acknowledged the breakdown bluntly. Dr. Jean-Jacques Muyembe, head of the National Institute of Biomedical Research, said the surveillance system simply had not worked, pointing to delays in both reporting the epidemic and processing diagnostic samples.
Why a Rare Virus Slipped Through
One of the central reasons for the delay was the unusual nature of the virus itself. The outbreak is caused by Ebola Bundibugyo, a rare species of the virus for which there are no approved vaccines or specific treatments.
Testing equipment available in Ituri was calibrated only for the most common strain, known as Zaire ebolavirus. As a result, early samples kept returning negative — falsely reassuring health workers that Ebola was not the culprit.
The pattern repeated itself. Samples collected in late April near the Ugandan border tested negative both locally and in Kinshasa. A later batch, gathered in early May south of Bunia, also tested negative in the field. Only when those samples were re-examined in Kinshasa did the truth emerge. Testing with a kit designed for yet another strain, Ebola Sudan, scientists were surprised to find the Bundibugyo species instead.
A Region Working Against the Response
Beyond technical hurdles, the geography and politics of Ituri made early detection extraordinarily difficult.
The outbreak’s epicenter is believed to be Mongbwalu, a busy gold-mining town that draws large numbers of migrant laborers. During the rainy season, the area is nearly impossible to reach. Several armed militias operate there, frequently clashing with one another and with the Congolese Army, which forces most health authorities to remain in Bunia, roughly 30 miles away.
That distance had deadly consequences. As Dr. Bill Kanyenche, a physician involved in the Ebola response in Bunia, explained, people were dying with clear signs of Ebola in their communities while neither residents nor local health workers recognized what they were seeing. He believes the outbreak should have been declared nearly a month earlier than it was.
The crisis also worsened because of community mistrust. Dr. Belizaire noted that some people may not have shared information or sought medical care, allowing the virus to spread further before officials had any idea of its presence.
The Human Toll Keeps Climbing
The numbers tell a grim and worsening story. According to the latest figures from the US Centers for Disease Control and Prevention, the outbreak in DRC has grown to 10 confirmed cases and 336 suspected cases, including 88 deaths. Uganda has reported two confirmed cases, one of them fatal, both linked to travel from Congo.
The disease has now been detected across nine health zones in Ituri Province. Cases have also reached far beyond the epicenter, including the capital Kinshasa and the eastern city of Goma, where an infected woman had traveled from Ituri.
The danger is amplified by the virus’s lethality. Bundibugyo carries a fatality rate of up to 50 percent. Many deaths have reportedly been linked to unsafe burial practices, where bodies are washed, touched, and wrapped without protective measures. In one especially alarming sign, four health care workers died within just four days at Mongbwalu General Referral Hospital.
An American doctor, Peter Stafford, is among the confirmed cases. The Christian missionary organization he worked with confirmed he was exposed while treating patients at a hospital southeast of Bunia. US authorities have since worked to move exposed Americans out of the country for care under quarantine.
A “Critical Four-Week Detection Gap”
The WHO has described a “critical four-week detection gap” between the onset of symptoms in the presumed first case and laboratory confirmation of the outbreak. The agency suggested health workers had a low index of suspicion for Ebola, possibly mistaking it for other illnesses circulating in the region, such as influenza-like infections and mosquito-borne diseases.
Experts have made clear how costly that delay could be. Atul Gawande, a former senior US Agency for International Development official, said the situation had clearly been out of control for weeks and stressed that speed is everything in containing Ebola. He added that the closure of USAID had already hampered the response.
Jean Kaseya, head of the Africa Centres for Disease Control and Prevention, described himself as being in “panic mode,” warning that people were dying while he lacked both medicines and vaccines.
A Race Against a Head Start
The Ebola outbreak in Congo now stands as a sobering example of how a single broken link in a surveillance chain can give a deadly virus a weeks-long head start. With no vaccine or treatment for the Bundibugyo strain, contact tracing made nearly impossible by conflict and displacement, and cases already crossing borders, the response faces extraordinary obstacles.
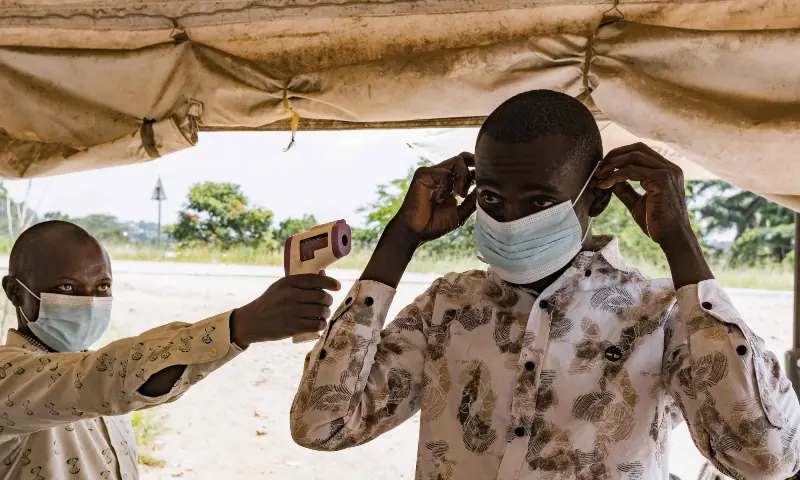
Five countries in the region have begun screening travelers or tightening border controls, and Rwanda has closed its border with Congo. Yet the fundamental challenge remains: health workers are now chasing a virus that was allowed to spread unseen. As officials have repeatedly emphasized, the earliest hours of an outbreak are the most critical — and in Ituri, those hours were lost long before anyone knew the clock had started.
This article discusses a serious public health emergency. For accurate, up-to-date guidance, readers should consult official sources such as the WHO and their national health authorities.
Author